







30-Y FOLLOW-UP OF A PU/AM INHALATION CASE
Christian Wernli
1,
*, Jost Eikenberg
1
, Olaf Marzocchi
2
, Bastian Breustedt
2
, Ursula Oestreicher
3
, Horst Romm
3
,
Demetrio Gregoratto
4
and James Marsh
4
1
Paul Scherrer Institute (PSI), Villigen, Switzerland
2
Karlsruhe Institute for Technology (KIT), Karlsruhe, Germany
3
Federal Office for Radiation Protection (BfS), Oberschleissheim, Germany
4
Public Health England (PHE), Harwell Science and Innovation Campus, UK
*Corresponding author: christian.wernli@alumni.ethz.ch
In 1983, a young man inhaled accidentally a large amount of plutonium and americium. This case was carefully followed until
2013. Since no decorporation measures had been taken, the undisturbed metabolism of Pu and Am can be derived from the data.
First objective was to determine the amount of inhaled radionuclides and to estimate committed effective dose. In vivo and excre-
tion measurements started immediately after the inhalation, and for quality assurance, all types of measurements were performed
by different labs in Europe and the USA. After dose assessment by various international groups were completed, the measure-
ments were continued to produce scientific data for model validation. The data have been analysed here to estimate lung absorp-
tion parameter values for the inhaled plutonium and americium oxide using the proposed new ICRP Human Respiratory Tract
Model. As supplement to the biokinetic modelling, biological data from three different cytogenetic markers have been added.
The estimated committed effective dose is in the order of 1 Sv. The subject is 30 y after the inhalation, of good health, according
to a recent medical check-up.
HISTORY OF THE INHALATION CASE
A first paper describing the details of the accident, the
early measurements and dose estimates of the Pu/Am
inhalation case of 1983 at the former Federal Institute
for Reactor Research in Switzerland has been pub-
lished in 2007
(1)
. Immediately after accidental inhal-
ation by a 26-y-old male technician, dose estimates
were of primary interest. The results of measurements
perf ormed in various la bs w er e used by sever al organisa-
tions for testing their internal dosimetry pr ogr ammes for
actinides. La ter on, this case became mainl y of scientific
interes t since no chela ting agent w as used and, ev en
after 30 y, in vivo and excretion measur ements wer e still
possible. Fortunatel y, the person concerned accepted
all these measurement procedur es. Over the last fe w
years, organ measurements were performed with
highly specialised instruments at Karlsruhe Institute
for Technology (KIT)
(2)
and the excretion measure-
ments were done again at Paul Scherrer Institute
(PSI)
(1)
.Inadditiontoallthephysicalmeasure-
ments, current cytogenetic analyses were performed
at Federal Office for Radiation Protection
(3)
to com-
plete scientific data by biological studies.
RECENT IN VIVO MEASUREMENTS
Instruments and method
Recent in vivo measurements have been performed at
KIT Karlsruhe using a system of four HPGe detec-
tors
(2)
. Two detector configurations were used: a
mixed one to monitor four organs (left lung, right
lung, liver and knee), and a configuration specific for
the skeleton (two detectors around the skull and two
detectors for the knees). The measurement time was
4000 s per configuration. The net area of the peaks
was estimated according to ISO 28 218. The calcula-
tion of the activity for
241
Am in each organ was per-
formed using both ICRP Man and ICRP Female as
calibration phantoms, and the calibration data were
obtained using MCNPX
(4)
after a validation of the
method
(2)
. The analysis of the data was performed first
for the mixed configuration; the results were used to
correct the calculations for the skeleton configuration.
The calculation of the activities in the mixed con-
figuration was not performed using each detector in-
dependently, because it is known that a measurable
part of the counts is generated by the crosstalk
between neighbouring organs and detectors. Instead,
the direct and the indirect contributions and the four
peak areas were used to write a system of linear equa-
tions. The solution of the system consisted of the ac-
tivity in each organ.
DISCUSSION
The solution of the system of equations applied to the
mixed measurement configuration produced a negative
value of
241
Am activity in the liver, independently from
the calibr ation phantom used, suggesting the la ck of
241
Am in the organ. The system was therefore rewritten
to exclude the liver and the solution calculated again.
The final data are shown in Table 1.
The activity in the lungs calculated using the mixed
configuration was used to correct the peaks recorded
in the detectors around the skull. This was performed
# The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.per missions@oup.com
Radiation Protection Dosimetry (2015), Vol. 164, No. 1–2, pp. 57–64 doi:10.1093/rpd/ncu342
Advance Access publication 19 December 2014

by simulating with MCNPX the counting efficiency
for photons originated in the lungs and reaching the
detectors around the skull. The number of counts ori-
ginated by the skeleton was therefore lowered: the net
value was 3– 5 % lower when using ICRP Male as
calibration phantom and 8–10 % lower for ICRP
Female. The different results can be explained by the
higher amount of muscles in ICRP Male that acts as
shield and lowers the cross-counting efficiency for the
detectors around the skull. The corrected activities
are listed in Table 2.
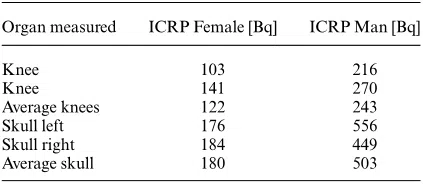
By comparing the results for the mixed detector con-
figur ation with the resul ts f or the skeleton configur ation,
it appears that the acti vity value f or the skeleton is co-
her ent only when using ICRP F emale: the calibration
with ICRP Man produces a discrepa ncy of 30 %.
A partial explanation for the issue is related to the
MCNPX simulations and the quality of the models
used to reproduce the detectors: currently, they are
optimised only for the front face, not for the photons
impinging on the sides of the crystal. More accurate
models will be available in the future.
The placement of the detectors relative to the
subject affects the results heavily, and it is the most
probable cause of the discrepancy between skull and
knees measurements. Additional simulations found
the efficiency for the skull to decrease by 50 % for a
2-cm slide of the subject down the reclined stretcher
[see the pictures in (2)]. The placement of the detec-
tors was checked at the beginning, but not at the end
of the measurement sessions; therefore, an accurate
correction factor for the measurements around the
skull is not possible. A similar issue may affect the
data for the knees, but the effect is an order of magni-
tude smaller: the simulations showed a decrease in the
counting efficiency of at most 7 % for a slide of 2 cm.
INTERPRETATION OF MEASUREMENTS
This inhalation case has been analysed in the past by
different authors and has been used in an internal
dosimetry inter-comparison exercise
(5)
. The analysis
did show a very long lung retention, which could only
in part be accounted for by assuming that the inhaled
material was very insoluble. A significantly slower
particle transport clearance mechanism in the lungs
had also to be assumed in order for the model predic-
tions to agree with the measurements.
The data have been analysed here, by using the fol-
lowing models:
† for deposition, particle transport and absorption
to blood in the respiratory tract, a revision of
the Human Respiratory Tract Model (HRTM)
(6)
.
In the revised particle transport model, the mater-
ial deposited in the alveolar compartment clears
to the bronchial tree at a rate of m
T
¼ 0.002 d
21
and to the interstitial compartment at a rate of
m
I
¼ 0.001 d
21
. The interstitial compartment
clears very slowly to the regional lymph nodes at
a rate of 0.00003 d
21
;
† for transit through the alimentary tract the ICRP-
30 model
(7)
;
† for systemic biokinetics, the Leggett model f or plu-
tonium
(8)
and the ICRP model for americium
(9)
.
The isotopic composition of the inhaled aerosol was
estimated from measurements in January 1983 (4
months before the accident) on the fuel samples used
in the solution that was overheated and spread out in
the accident. The alpha activity composition is
recorded as 10 %
241
Am, 9 %
238
Pu, 55 %
239
Pu and
26 %
240
Pu. The
241
Pu (beta) activity is 750 % of the
total alpha activity. The uncertainty on these mea-
surements is not known. The above isotopic compos-
ition is consistent with the activity ratio (
238
Pu þ
241
Am)/(
239
Pu þ
240
Pu) ¼ 0.24 + 0.05 calculated
from the early faecal samples. There are no faecal
measurements for
241
Pu, but a previous laboratory
record gives the
241
Pu activity as 655 % of the total
alpha activity whereas all the alpha activities are
within a few per cent from the values given above. The
reason of the discrepancy for
241
Pu is not known.
As in the previous analysis, an effective AMAD
(10)
(Activity Median Aerodynamic Diameter) of 5 mm
has been estimated from early lung and early faecal
excretion data (including the activity that would have
appeared in the faeces if it had not been not removed
with a nasal swab and a bronchial slime before the
first chest measurement was done
(1)
). This value has
been used to calculate the fractions of material
Table 1. Activities calculated for the mixed configuration,
according to the calibration phantom used.
Organ ICRP Female [Bq] ICRP Man [Bq]
Skeleton
a
152 288
Lung left
b
60 73
Lung right
b
59 77
Liver 0 0
a
Based on knee measurements.
b
The calibration phantom did not distinguish between lung
and thoracic lymph nodes.
Table 2. Activities calculated for the skeleton-specific
configuration, according to the calibration phantom used.
Organ measured ICRP Female [Bq] ICRP Man [Bq]
Knee 103 216
Knee 141 270
Average knees 122 243
Skull left 176 556
Skull right 184 449
Average skull 180 503
C. WERNLI ETAL.
58

deposited in each of the lung regions. The calculated
activity deposited in the nasal region has been
adjusted by subtracting the amount that was removed
immediately after the intake by nose swab. This cor-
rection does not affect the estimate of the effective
dose but only the fit to the very early faecal data.
Particles deposited in the lungs are cleared by two
competing mechanisms, by particle transport (to the
gut and to the l ymph nodes) and b y absorption to
blood of the dissolving ma terial. For the latter, f
r
indi-
cates the fraction dissolved rapidly at the rate s
r
,
whereas the complementary fraction (1 2 f
r
)isdis-
solv ed slowly at the rate s
s
. A fra ction f
b
of the dissolved
material may not be absorbed directly into blood and
could bind temporaril y (s
b
. 0) or permanentl y (s
b
¼
0) to lung tissues. As mentioned, the fra ction (1 2 f
b
)is
availabletobeabsorbedtobloodattheratess
r
and s
s
.
Absorption of material fr om the respiratory tra ct to
blood wa s shown to be slo w in pre vious analy sis. The
inhaled material was initiall y assumed to be ‘type S’
solubility
(11)
, with absorption parameter values: f
r
¼
0.001, s
r
¼ 1d
21
, s
s
¼ 0.001 d
21
, and a bound state
was assumed with f
b
¼ 0.002 and s
b
¼ 0d
21(6, 12)
.
Note that the bound state does not play a significant
role in the long-term retention in the lungs because
the material is relatively insoluble. The gut uptake
fraction was kept fixed to its default value of f
1
¼ 5
10
24
for type S material.
Measurement err ors wer e assumed to be log-normally
distrib uted. The geometric standard devia tions, or sca tter -
ing factors , for the differ ent da tasets wer e either estima ted
from the data, as described by Marsh et al.
(13)
,or
based on the default values given in the IDEAS
guidelines
(10)
. The values for the scattering factors were
1.2, 1.6 and 2.4 for chest, urine and faecal measure-
ments and 2 for liver and skeleton.
The agreement between measurements and model
predictions was poor when using default parameter
values, and the following changes to the models were
introduced to improve the fit to the data:
† the particle transport in the alveolar–interstitial
region was reduced;
† the absorption parameter values of the inhaled
material were optimised, either assuming that
they were the same for Am and Pu (i.e. shared
values) or that they were different (i.e. independ-
ent);
† the isotopic activity composition was allowed to
vary;
† the transfer rates from blood to urinary bladder
were varied in order to improve the fit to the skel-
eton and liver measurements.
The changes were applied by finding optimal model
parameter values using the maximum-likelihood
method. To address first the issue of activity balance,
only chest and excretion data were used. Liver and
skeleton data were included only in the last stage of
the optimisation. The agreement between model pre-
diction and measurements improved significantly, in
terms of chi-squared, for each of the above changes
(Table 3).
The adoption of the revised HRTM model
(6)
improves the fit to lung and faecal excretion data,
compared with the previous HRTM
(11)
, but a further
reduction of the particle transport rate from the al-
veolar region to the bronchiolar needs to be applied,
from m
T
¼ 2
`
10
23
d
21
to m
T
¼ 3
`
10
24
d
21
. The
optimal value for the rate to the interstitial regions
(m
I
¼ 8.5
`
10
24
d
21
) differs only slightly from the
default value (m
I
¼ 1
`
10
23
d
21
). The changes may
also be expressed as an increase of the so-called
sequestered fraction in the alveolar– interstitial
region, m
I
/(m
I
þ m
T
) from 0.33 to 0.74 and in the
slowdown of the clearance to the gut. This value is
relatively high but close to the upper limit of the 68 %
probability range for the inter-subject variation: (0.2,
0.7)
(14)
. Assuming that americium is more soluble
than plutonium in the lungs improves the overall pre-
diction for urine excretion, although the very late
americium excretion remains slightly overestimated.
The rapid and slow absorption rates s
r
and s
s
for plu-
tonium are not well determined by the data, and it
would be possible to assume the same values of s
r
and
s
s
(shared values) for both Am and Pu without affect-
ing significantly the fit to the data. However, a much
better fit is obtained when the values for the rapid
fraction f
r
are optimised independently. The optimal
shared values are s
r
¼ 0.2 d
21
and s
s
¼ 5
`
10
25
d
21
,
and f
r
¼ 0.0014 for Pu and f
r
¼ 0.05 for Am. The
result might be interpreted as an indication that
Table 3. Lung absorption parameters, committed effective
dose (CED) and organ doses (equivalent doses and per cent
contribution to the effective dose) for each added changes in
the optimisation.
PT þ
AbsP
þ isotopic
composition
þ Blood–
UB
f
r
(Pu) 0.0014 0.0017 0.004
f
r
(Am) 0.05 0.04 0.08
s
r
(d
21
) 0.21 0.19 0.32
s
s
(10
25
d
21
)5 5 7
CED (Sv) 1.3 1.1 1.2
Lung
[Sv (%)]
8.3 (77) 6.8 (74) 6.3 (67)
Liver 2.3 (7) 2 (7) 3 (10)
Bone surface 10 (8) 9 (8) 14 (12)
R.B.M. 0.5 (5) 0.5 (5) 0.7 (7)
x
2
TOT
(236 data)
261 232 212
a
x
2
LUNG
(17 data)
38 16 12
a
242 data, including skeleton (3) and liver (3) data.
30-Y FOLLOW-UP OF A P
U/AM INHALATION CASE
59

initially americium dissolves faster. Americium oxide
is generally more soluble than plutonium oxide
(15)
,
but it is usually also considered that the rate at which
a particle dissociates is determined by the particle
matrix and therefore the dissolution parameter values
for americium and plutonium should be similar if
they belong to the same matrix. An interpretation of
the above result could possibly be provided by a better
knowledge of the physicochemical properties of the
inhaled material.
The overall fit is not sufficiently good, and this is
mainly due to the model prediction being ‘pulled’ in
opposite directions by chest and urine data.
An estimate of the isotopic composition of the
inhaled material is necessary to determine the initial
amount of americium and plutonium (isotopes)
deposited in the lungs. The values given above have
been considered as fixed in previous analysis. Based
on the available information, the authors assumed
here a relative error of 10 % and used it for a con-
strained optimisation. This would be equivalent to
introduce a prior distribution for the isotopic frac-
tions within a Bayesian framework.
The result of the optimisation, 13 %
241
Am, 9 %
238
Pu, 53 %
239
Pu, 25 %
240
Pu and 660 %
241
Pu,
shows that the complete set of data and the models
used might be more consistent with a different isotop-
ic composition. However, the ratio (
238
Pu þ
241
Am)/
(
239
Pu þ
240
Pu) ¼ 0.25 is still compatible with the es-
timate 0.24+0.05 based on the early faecal measure-
ments. The lower beta activity (
241
Pu) also cannot be
completely excluded because of the two different
values given in the laboratory records.
The previous adjustments to the models improve
significantly the overall agreement between model
prediction and experimental data, except for liver and
skeleton. The reasons for the discrepancy could be
various, but to improve the fit to the liver and skeleton
data, it is necessary to modify systemic parameter
values. A sensitivity analysis shows that reducing the
amount transferred from blood to bladder is the most
effective in ensuring a good fit to the two systemic
organ datasets and improving further the agreement
with the urine data. The main effect is an increase of
the dose to internal organs, because more activity is
retained in the body instead of being excreted through
urine, and an adjustment of the lung absorption para-
meters. Note that this effect is achieved even if liver
and skeleton data are not included in the fitting
because it is mainly driven by the urine data. The rates
from blood to urinary bladder have been changed by
keeping constant the removal half-time from blood. A
constraint equivalent to a lognormal prior distribution
with geometric standard deviation equal to log(1.7)
(16)
has been applied in the optimisation.
Table 3 shows how the optimal parameter values,
doses and chi-squared did vary when the changes [ par-
ticle transport (PT) plus absorption parameters (AbsP),
isotopic composition, blood to urinary bladder] w e r e
app lied sequentially.
LUNG ABSORPTION PARAMETERS
The maximum-likelihood procedure used for the
parameters estimation indicates that the shared par-
ameter s
r
and f
r
for Pu are less well defined by the
data than the other parameters. The estimates of f
r
, s
r
and s
s
are not significantly correlated between them
(j
r
j , 0.15) but show higher correlation with the esti-
mate of the blood-to-urinary bladder rate.
The uncertainty on the estimates of the lung ab-
sorption parameters has been further investigated by
using Bayesian Markov chain Monte Carlo sam-
pling
(17)
. Lognormal prior distributions have been
assumed for the parameters, which were constraint in
the optimisation. ‘Non-informative’ priors (normal
distribution for the log-transformed variable with
s
¼ 2 and centred on the best-fit result) have been
used for all the other parameters. Most of the absorp-
tion parameters were well defined (Table 4) as the pos-
terior distribution was relatively narrow (compared
with the prior distribution) and approximately
centred on the best-fit value. The exceptions are the
fast-absorbed fraction f
r
for plutonium, for which
only an upper limit ( f
r
, 0.015) is clearly defined,
and for the shared parameter s
r
for which the lower
limit is better defined than the upper limit (s
r
. 0.2
d
21
). All set of measurements used in the analysis are
given in the Annex (Tables A1– A5). Figures 1–4
show measurements and best-fit model predictions for
a subset of the datasets. As shown in Figure 1,mostof
the
241
Am activity predicted in chest at later times is
due to in-growth from
241
Pu.
CYTOGENETIC ANALYSIS
In addition to the biokinetic modelling, three differ-
ent cytogenetic assays have been performed to analyse
diverse biomarkers of exposure in blood lymphocytes.
Dicentric assay
Up to now, the conventional analysis of dicentric
chromosomes (dicentric assay) is the most appropriate
Table 4. MCMC results for lung absorption parameters
and CED.
Mean value 95 % probability interval
f
r
(Am) 0.08 0.04–0.12
f
r
(Pu) 0.003 ,0.015
s
r
(d
21
) 0.4 0.17–5
s
s
(d
21
)8
`
10
25
6
`
10
25
–1
`
10
24
CED (Sv) 1.2 1.0–1.35
C. WERNLI ETAL.
60

assay to estimate a dose in case of an acute irradi-
ation
(18, 19)
. This assay was also used in a previous
examination of the same person years ago
(1)
. In the
present study, a total of 1000 cells from Giemsa
stained slides were analysed. The observed frequency
of 2 dicentric chromosomes per 1000 cells was not sig-
nificantly different ( p . 0.05) in comparison with the
authors’ control value of 1.15 dicentric chromosomes
per 1000 cells. This result was to be expected because
of the 30-y time period between the first accidental
exposure and the current blood sampling. The bio-
logical half-life of lymphocytes with dicentric chro-
mosomes is assumed to be 3 y. Due to a detriment of
dicentric chromosomes during cell division, the yield
of lymphocytes in the circulating blood bearing this
biomarker will decrease in the course of time.
FISH assay (symmetrical translocations)
The yield of symmetrical translocations in 3017 cells
scored was significantly increased (23.8+5.0/1000
cells, FG (Genome equivalents) values) in compari-
son with an age-adjusted control group including 35
persons and 88 934 cells scored [7.5+0.51/1000 cells,
FG (Genome equivalent) values]. This aberration
type has the advantage to pass cell division without
major detriment and thus is more persistent. In conse-
quence , s ymmetrical a berra tions ar e the indica tor of
choice f or past and chronic radiation conditions
(20)
.In
the curr ent case, the significantincreaseofsymmetrical
translo cations indica tes an irradiation incident. Because
of the la ck of an appropriate dose–ef fect curve f or this
radiation quality (alpha particles) and the extreme long
time period since the exposur e, a dose r econs truction
wa s consider ed to be not feasible.
Figure 4.
239
Pu þ
240
Pu in 24-h faecal excretion.
Figure 1.
241
Am in chest. The dash-dotted curve shows the
predicted
241
Am activity without taking into account of
in-growth from
241
Pu.
Figure 2.
241
Am þ
238
Pu in 24-h urine excretion.
Figure 3.
239
Pu þ
240
Pu in 24-h urine excretion.
30-Y FOLLOW-UP OF A P
U/AM INHALATION CASE
61